Anti-Obesity Drug Compartmental PK Analysis Service
InquiryThe global obesity epidemic necessitates the rapid development of safe and effective anti-obesity medications (AOMs). However, the complex physiological changes associated with obesity, such as altered body composition, increased adipose tissue, and chronic inflammation, significantly impact how drugs are absorbed, distributed, metabolized, and excreted (pharmacokinetics or PK). This variability poses unique challenges for determining optimal dosing and ensuring patient safety.
Obese Phenotype Pharmacokinetic Mapping
At Protheragen, we leverage two decades of expertise to address this critical translational gap. Our anti-obesity drug compartmental PK analysis service provides an advanced, model-informed approach to accurately characterize the Absorption, distribution, Metabolism, and Excretion (ADME) of novel therapeutics in preclinical models of obesity. By moving beyond traditional non-compartmental analysis (NCA), we offer deep, mechanistic insights into drug disposition, essential for successful preclinical-to-clinical translation and the reduction of expensive late-stage failures. This specialized service is strictly focused on generating high-quality preclinical data to inform your drug candidate's profile.
Core Technologies: Mechanistic Modeling of Complex Tissue Dynamics
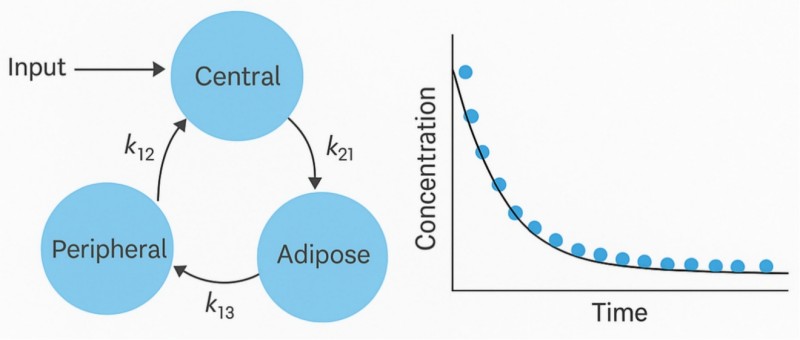
The primary strength of our service lies in implementing sophisticated multi-compartment PK Modeling that explicitly accounts for the unique physiology of the obese state. We do not just calculate plasma half-life; we structurally model the drug's partitioning into relevant physiological compartments. Key technological differentiators include:
- Advanced Compartmental Modeling
We utilize non-linear mixed-effects (NLME) modeling to accurately fit concentration-time data from Preclinical Models (e.g., diet-induced obese rodents) to complex, tailored compartmental structures. This allows for precise estimation of micro-constants governing distribution and elimination.
- Adipose Tissue Heterogeneity
Recognizing that adipose tissue is not a single, monolithic compartment, our models incorporate partitioning ratios and tissue-specific blood flow parameters, particularly crucial for understanding the sequestering and delayed release of highly lipophilic anti-obesity agents. The literature confirms that understanding tissue-specific PK, especially within fat depots, is vital for accurate translational prediction.
- Clearance Pathway Deconvolution
Obesity can alter the activity of drug-metabolizing enzymes (CYP isoforms) and transporters. Our models are designed to deconvolve hepatic and renal clearance components, linking changes in these parameters directly to the observed systemic PK in obese preclinical models. This allows developers to understand if clearance changes are due to metabolic capacity or altered tissue perfusion.
- Integration with Bioanalytical Precision
We pair our modeling expertise with state-of-the-art bioanalytical quantification of parent drug and active metabolites in preclinical matrices (plasma, liver, target tissues, specific adipose depots) to ensure the highest data quality input for robust model fitting.
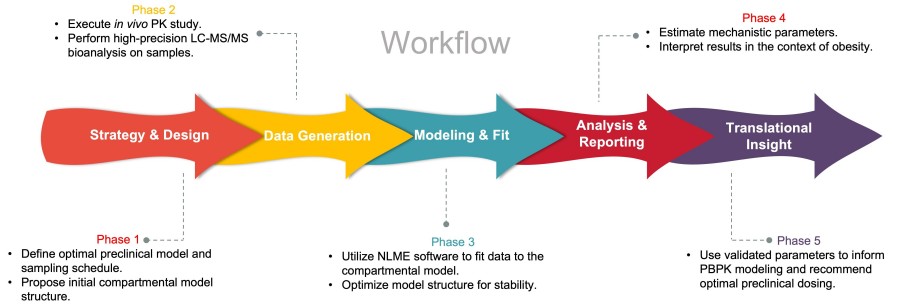
Workflow: A Structured Path to PK Insight
Protheragen's compartmental PK analysis is delivered through a rigorous, client-centric, and fully compliant preclinical workflow, ensuring actionable insights at every stage.
Fields of Application
This service is critical for a wide range of therapeutic candidates where body mass and composition are major covariates influencing drug exposure.
- Anti-Obesity Therapeutics (OTs)
Small Molecules or peptide agonists/antagonists where tissue-specific distribution (especially Vd in adipose tissue) dictates efficacy and safety.
- Metabolic Syndrome Drugs
Candidates targeting type 2 diabetes (T2D), non-alcoholic steatohepatitis (NASH), or dyslipidemia.
- Any Highly Lipophilic or Basic Compound
Drugs where physicochemical properties suggest significant tissue partitioning and susceptibility to body composition changes.
- Combination Therapies
Understanding the precise PK of individual components to optimize fixed-dose ratios.
Advantages: Unmatched Expertise in Obesity PK
Choosing Protheragen means partnering with a team that transforms complex ADME challenges into clear strategic advantages.
Deep Mechanistic Understanding
We move beyond descriptive NCA data, providing a mechanistic compartmental map of your drug's fate. This insight is crucial for predicting potential drug-drug interactions (DDIs) or PK variability across different obesity phenotypes.
Mitigation of Translational Risk
By accurately modeling the effect of altered body composition and fatty liver on Vd and CL, our service minimizes the risk of unexpected PK behavior in subsequent clinical stages. Published data demonstrate Protheragen's success in accurately predicting Vd and clearance adjustments for highly lipophilic compounds in preclinical models, which is critical given the complexity of drug partitioning in expanded adipose tissue.
Accelerated Candidate Selection
Precise PK data allows for rapid winnowing of candidates and informed optimization of chemical structure early in the discovery phase, saving time and resources.
Enhanced Confidence Through Data Quality
Our rigorous methods and detailed reporting generate robust compartmental models, providing compelling, high-quality evidence that strengthens the foundation of your drug candidate's preclinical profile and accelerates its progression toward the next development milestone.
Contact Protheragen to discuss a customized compartmental PK study.
Service ScopeThe Protheragen service is specialized for the preclinical phase of drug discovery and development. Our core offerings include:
Compartmental PK in Lean vs Obese Preclinical Models
We design and analyze PK studies comparing lean and obese animals across:
- Oral, subcutaneous, intraperitoneal, or IV routes
- Single ascending and multiple-dose paradigms
- Standard chow vs high-fat diet conditions
This enables a quantitative dissection of how obesity alters absorption, distribution, and systemic clearance.
Adipose Distribution and Long-Tail Kinetics Assessment
For lipophilic candidates, we support:
- Tissue PK profiling with emphasis on adipose tissue, liver, and muscle
- Extended sampling to characterize context-sensitive half-lives and late elimination phases
- Compartmental and PBPK models that explicitly represent adipose reservoirs and delayed wash-out, drawing on the trap-compartment and memory-aware frameworks described in recent literature.
Obesity-Aware Oral Absorption Modeling
Building on evidence that gastric emptying and GI transit are altered in obesity, we quantify the impact of:
- Formulation properties (solubility class, dissolution rate)
- Fed vs fasted conditions and high-fat diets
- Transit-time changes on Cmax, tmax, and AUC in obese vs lean animals
Population PK and Covariate Analysis Across Body Composition
Our models incorporate:
- Continuous covariates (total body weight, lean mass, fat mass)
- Categorical obesity status or diet groups
- Potential interactions with age or sex, where study designs allow
This reveals whether exposure differences are primarily driven by fat vs lean mass, perfusion, or clearance changes.
Preclinical PBPK for Obesity and Cross-Species Scaling
Where needed, we build PBPK frameworks that:
- Integrate obesity-specific organ sizes and blood flows
- Explore exposure changes across a wide "BMI-equivalent" range for the species
- Provide mechanistic insight that complements empirical compartmental PK
Reach out to discuss whether a PBPK-enhanced package is appropriate for your stage.
Publication Data
Title: Pharmacokinetics, Tissue Distribution, and Anti-Lipogenic/Adipogenic Effects of AllylIsothiocyanate Metabolites
Journal: PLoS ONE, 2015
DOI: https://doi.org/10.1371/journal.pone.0132151
Summary: This study investigates the pharmacokinetics, tissue distribution, and anti-lipogenic/adipogenic effects of allyl-isothiocyanate (AITC) metabolites. AITC, an organosulfur phytochemical abundant in cruciferous vegetables (e.g., mustard, wasabi), is primarily metabolized via the mercapturic acid pathway, but its metabolites' biological functions and pharmacokinetic profiles remain unclear. Using liquid chromatography-tandem mass spectroscopy (LC-MS/MS) and high-performance liquid chromatography (HPLC), the researchers identified two primary AITC metabolites in rats—glutathione-conjugated AITC (GSH-AITC) and N-acetylcysteine-conjugated AITC (NAC-AITC)—and synthesized them to study their in vitro activity and in vivo disposition.
Key Findings
- AITC Metabolites: AITC is fully metabolized in rats via the mercapturic acid pathway to two main metabolites (GSH-AITC, NAC-AITC); no intermediate metabolites were detected.
- Pharmacokinetics: Both metabolites absorb rapidly (Tmax = 0.5h in plasma); NAC-AITC is the dominant circulating metabolite (10×higher Cmax/AUC vs. GSH-AITC) and is primarily excreted in urine (GSH-AITC is undetectable in urine).
- Tissue Distribution: GSH-AITC accumulates most in the liver (then kidney/spleen/heart/lung); NAC-AITC concentrates in the kidney; distribution aligns with organ blood perfusion rates.
- Anti-Adipogenic Activity: Dose-dependently suppress 3T3-L1 preadipocyte differentiation by reducing adipogenesis markers (PPAR-γ, C/EBPα, FAS) and inhibiting mTORC1 (via lower S6K1/4EBP1 phosphorylation).
- Anti-Lipogenic Activity: Reduce oleic acid-induced lipid buildup in hepatocytes by downregulating lipogenic proteins (FAS, SREBP-1c) and activating AMPK.
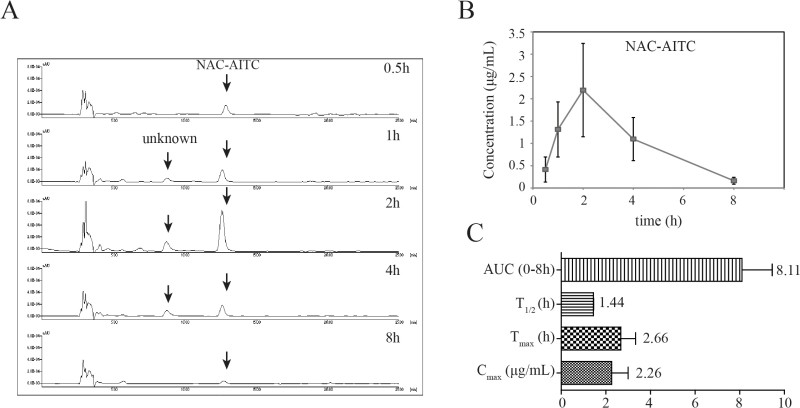 Fig.1 Pharmacokinetic analysis of GSH-AITC & NAC-AITC in rat urine. (Kim, et al., 2015)
Fig.1 Pharmacokinetic analysis of GSH-AITC & NAC-AITC in rat urine. (Kim, et al., 2015)
Customer Review
Metabolic Diseases, Biotech Company (Preclinical Stage)
"We approached Protheragen with a lipophilic oral small molecule that behaved unpredictably in our obese rodent models. Their team built lean vs obese compartmental models, added an adipose trap compartment, and simulated multiple regimens for our efficacy and safety studies. The analysis revealed that our initial dosing schedule would have led to substantial accumulation in high-fat animals. With their guidance, we re-designed the regimen and avoided unnecessary repeat experiments. We now use their PK modeling reports as a standard component of our internal stage-gate reviews."
Dr. J. W., Director of Metabolic Diseases
Anti-Obesity Portfolio, Mid-Sized Pharma
"We approached Protheragen with a first-in-class small molecule and very aggressive timelines. They quickly proposed a staged biliary excretion program, coordinated analytics, and delivered a report that our board and investors could understand at a glance. The integration of experimental data with modeling was especially valuable. Based on this experience, we have already engaged them for transporter studies and PBPK support on our next candidate, and we expect this collaboration to continue as our pipeline grows."
Dr. J. L., Head of DMPK
Frequently Asked Questions
-
Can we use this service if we only have a single-dose PK study in obese animals?
Yes. A well-designed single-dose study can already support compartmental modeling, including lean vs obese comparisons. For long-tail or accumulation questions, we may recommend an additional repeat-dose experiment, which we can help design.
-
Do you handle both small molecules and peptides?
We routinely model small molecules and peptides. The model structure and parameterization differ—particularly around absorption and distribution—but the overall workflow (data QC, model fitting, simulation) is similar. Highly polar or large molecules may not require adipose trap compartments, and we will reflect that in the model choice.
-
What preclinical data do you need to start?
At minimum, we need PK concentration–time data (with sampling extending into the elimination phase), dosing details, animal metadata (body weight, sex, strain, obesity model), and analytical method information. Body composition, tissue PK, and biomarker data strengthen and refine the models but are not mandatory.
-
How do you distinguish the effect of obesity from other covariates?
We use population PK methods that explicitly test obesity-related covariates (body weight, fat mass, obesity status) alongside other factors such as dose level or sex. This helps separate true obesity effects from confounding and quantifies their contribution to clearance and Vd.
-
Can your models be used directly for clinical dose selection?
Our work is strictly preclinical. However, the outputs—such as obesity-adjusted exposure predictions, adipose trapping assessments, and PBPK frameworks—are structured so that clinical pharmacology teams can build on them when designing first-in-human and later-phase studies.
-
What if our compound shows no obvious differences between lean and obese animals?
That is still valuable information. Models that confirm minimal obesity impact are powerful when justifying simpler dosing strategies and can reduce the need for extra complexity in later development. We will document these findings clearly in our reports.
-
How do you ensure that advanced models (e.g., trap or fractional) are not overfitting?
We start from the simplest adequate structure and only introduce additional compartments or memory terms if strongly supported by diagnostics, long-tail behavior, and mechanistic plausibility. Model selection is guided by goodness-of-fit, predictive checks, and parsimony.
-
What is the typical timeline for a compartmental PK analysis project?
Timelines depend on data volume and model complexity. As a benchmark, lean vs obese single-dose PK modeling is often completed within a few weeks once curated data are in place. We can provide a more precise estimate once we review your dataset via our inquiry channel.
-
How do we get started, and what information should we include in our inquiry?
A concise description of your compound class, target mechanism, available PK data (species, regimens), key questions (e.g., adipose trapping, regimen design), and desired decision dates is ideal. Our team will respond with a proposed modeling scope and a list of any additional data that would enhance the analysis.
How to Contact Us
In the race to develop impactful anti-obesity therapies, preclinical teams cannot afford delays or ambiguous data—dead ends derail pipelines, and missed PK insights sink promising candidates. ABC's anti-obesity drug compartmental PK analysis service is purpose-built to empower discovery teams to move faster with unshakable confidence, delivering scalable, reproducible, decision-ready compartmental PK insights that complement modern obesity hit-finding strategies and accelerate lead optimization.
Online Inquiry Form: Contact Protheragen
Email: info@obesityscientific.com (Please include a short description of your compound class, current data, and key project questions)
Phone: 1-631-506-1393
Reference
- Kim Y.J.; et al. Pharmacokinetics, Tissue Distribution, and Anti-Lipogenic/Adipogenic Effects of Allyl-Isothiocyanate Metabolites. PLoS ONE. 2015, 10(8): e0132151. (CC BY 4.0)
All of our services and products are intended for preclinical research use only and cannot be used to diagnose, treat or manage patients.